Keto Lifestyle
Ketogenic diet therapy for diabetes
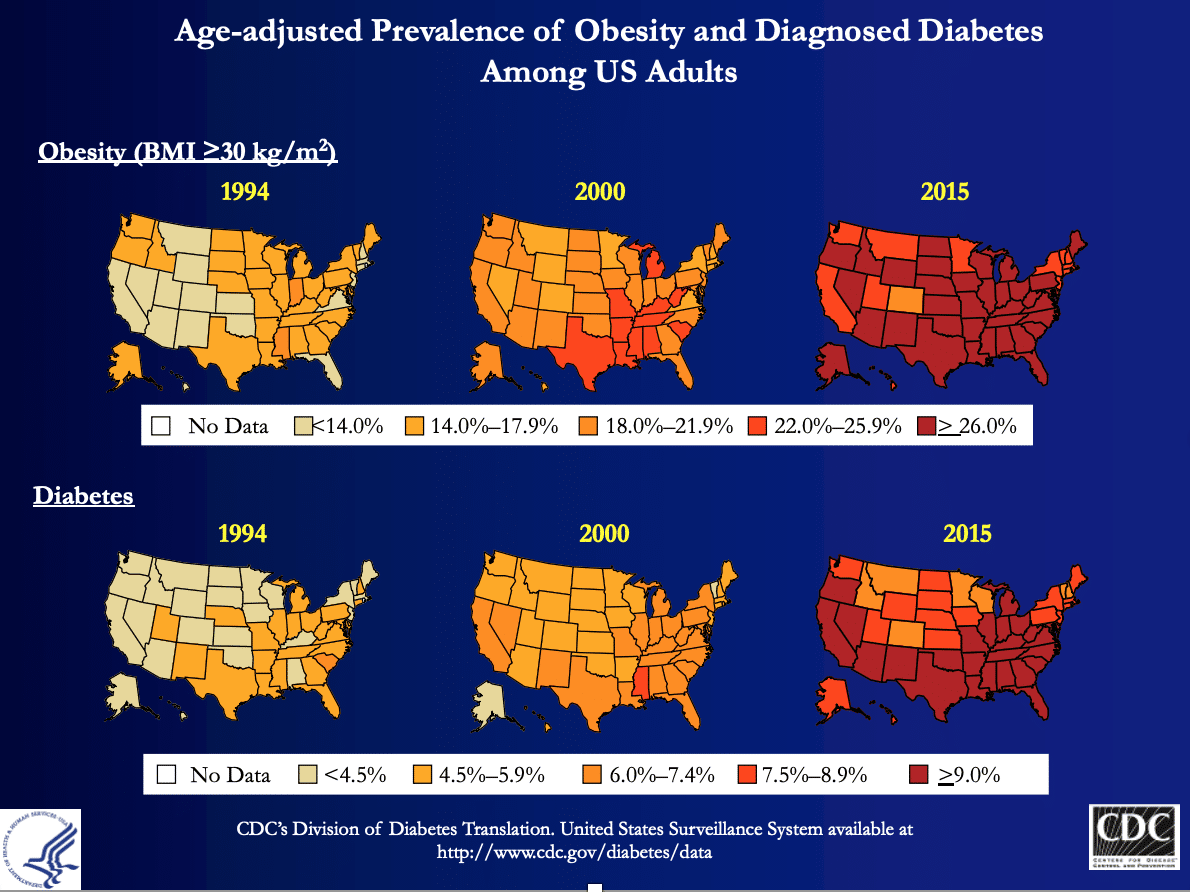
According to the Center for Disease Control (CDC) in Atlanta, Georgia, the number of people who are diagnosed with diabetes continues to rise and is considered an epidemic here in the USA as well as in many other countries. The incidence of diabetes closely follows the incidence of obesity. As you can see from the maps below, these increases have skyrocketed since 1994. We’ve written this blog to support the option of dietary therapy for a condition that has been primarily treated with medications.
Written by Kristi Storoschuk, Beth Zupec-Kania and Dr. Dominic D’Agostino
What is Diabetes?
Diabetes is a disease of faulty carbohydrate metabolism. It is characterized by the failure to properly regulate blood glucose levels. This disease involves a unique hormone called insulin. Insulin releases into the blood after there is an increase in blood glucose triggered by eating. Think of insulin like the fluid in your cars’ windshield washer. You squirt it out when you need it to clean debris on the window. Insulin squirts out as it is called upon to move glucose from the blood and into our cells where it is further modified to make energy. Excess glucose in our blood is unhealthy and requires more insulin. This is where the problem lies. Over time, the organ that squirts out insulin, the pancreas, starts to give out due to excessive wear. Similar to constantly pushing the button for the windshield fluid – eventually the button will wear out, or you’ll run out of fluid or both.
Before going any further let’s define the two different types of diabetes: Type-1 diabetes and Type-2 diabetes.
Type-1 Diabetes:
About 5% of people with diabetes have Type-1. This type is considered an autoimmune disorder where the body’s own immune system targets and attacks pancreatic beta-cells, ultimately destroying them. This is similar to how our immune system targets a virus or bacteria to protect us from harm, only it’s mistakenly removing something critically important to the body. These pancreatic beta-cells are where insulin is produced and released, and are required for healthy blood glucose regulation. Type-1 diabetics may still retain insulin sensitivity, however they require medicinal insulin to compensate for not being able to produce it themselves. Currently, there is no available cure for type-1 diabetes, but we argue there are better ways to manage this disorder then what is currently recommended.
Type-2 Diabetes:
Type-2 Diabetes is considered a disease of insulin resistance. Insulin resistance is when our cells fail to respond to insulin. When our cells can’t respond to insulin, the glucose in our blood has nowhere to go and builds up. Worse, our pancreas responds by making more insulin. This can keep blood glucose in a normal range for a while, however over time, even up to many years, can lead to type-2 diabetes – a state of consistently high blood glucose AND high insulin levels. Type-2 diabetics are typically diagnosed during adulthood, however, children are being diagnosed at an alarming rate. Unlike type-1 diabetes, type-2 diabetes can be reversed or at least put into remission, and there is a growing body of evidence to support this.
The Problem with Current Dietary Guidelines for Diabetes
Dietary recommendations for both type-1 and type-2 diabetes are made by the American Diabetes Association (ADA). Most patients are recommended to consume high-carbohydrate, moderate protein, low-fat diets. This dietary strategy requires diabetic medications to manage the glycemic effect of the diet instead of focusing on reducing glucose levels consistently. The ADA has recently included mention of low-carbohydrate diets in their 2018 recommendations but continues to support mainly high-carbohydrate, low-fat diets.
Why is a low-fat, high-carbohydrate diet a problem?
Unfortunately, the voice for low fat diets is louder than the evidence to support it. Currently medications have become the first line of care, secondary to, or in complete replacement of dietary changes. This approach treats the symptom (high glucose) instead of the cause (high-carbohydrate, low-fat diet). Diets that are high in carbohydrate and low in fat not only encourage high glucose levels but because fat lowers how quickly glucose is absorbed into the blood, there is the added effect of spikes in glucose throughout the day. This is referred to as glycemic control.
The goal of any diabetes intervention is to achieve glycemic control (especially less variability), but the reality is, that both type-1 and type-2 diabetics rarely achieve this with the current recommendations. To add to this, patients are often faced with the various side effects of diabetes medications and consequences of poor glycemic control. Frequent fluctuations between hypo- and hyperglycemic states can be extremely dangerous, and puts individuals at risk for several macro- and microvascular complications, in addition to other life-threatening consequences. It should also be noted that there is a bounty of emerging evidence linking continuously elevated insulin to almost all chronic diseases, and therefore a disease that requires the administration of insulin warrants caution. Finding a strategy that reduces the amount of insulin required to manage blood glucose levels is not only practical but could also be very protective.
Carbohydrates and Diabetes
Carbohydrate is the feed energy source with the strongest influence on blood glucose and insulin. In other words, dietary carbohydrate has the largest contribution to a rise in blood sugar. If diabetes is a problem of both elevated blood glucose and elevated insulin, it seems counterproductive for a diabetic to consume a high carbohydrate diet.
More carbohydrates = more glucose = more insulin
In 1928, it was discovered that you could increase the carbohydrate content of your diet as a type-1 diabetic, as long as you increased the dosing of insulin [1]. However, this is not a solution without consequence. It turns out that the greater the insulin load, the more room for error, and the potential for dangerous fluctuations in blood glucose, both accompanied by acute and chronic side effects. Type-1 diabetes is extremely difficult to manage due to various factors that influence the daily variations in blood glucose levels. These individuals are expected to calculate each dose of insulin to the requirements of each meal, which takes into consideration these various factors, including the carbohydrate load of the diet. Correctly identifying how much insulin is needed for a given meal takes precision beyond the scope of what most patients understand or can manage and simply the more insulin required, the greater the chance for blood glucose mistakes.
For type-2 diabetics, consuming carbohydrates typically requires anti-glycemic medications, or if severe enough, the addition of insulin. Type-2 diabetics also run the risk of hypo- and hyperglycemic events and their downstream consequences. Unfortunately, it’s more common for practitioners to use the word “management” than to discuss the possibility of remission. This puts patients that are highly motivated to make lifestyle changes in the passenger seat, but these patients deserve to have access to this information and be in the driver’s seat.
No one is going to make the changes they need if they are never presented with them as an option. And the lifestyle choice we are referring to is a ketogenic diet.
The Ketogenic Diet for Diabetes
The ketogenic diet for diabetes is not a recent idea [2], rather, a therapeutic approach that fell by the wayside following the discovery of insulin in 1921. Before insulin, carbohydrate restriction was commonly prescribed to diabetics, a story similar to the use of anti-epileptic drugs for epilepsy. Insulin was the breakthrough discovery that today enables type-1 diabetics to live with their disease, though we strongly believe the diet still plays a powerful role. As with most dietary interventions, the ketogenic diet receives pushback (specifically for type-1 diabetes) and therefore the research is limited to smaller subsets of patients, but exists nonetheless. This is in stark contrast to the complete lack of evidence to support the current dietary recommendations, a diet of which resembles the standard US Dietary Guidelines for all Americans.
Rationale for Ketogenic Diet for Diabetes
It is well established that foods with lower glycemic indices produce lower after-meal glucose and insulin responses. When you follow a ketogenic diet you naturally consume very low glycemic foods. The lower the surge in blood glucose following a meal, the easier it can be for a diabetic to manage. Moreover, the major feature of both type-1 and type-2 diabetes is impaired carbohydrate metabolism, supporting the rationale for carbohydrate restriction. Note: dietary protein has a small effect on blood glucose, dietary fat produces no effect but slows down digestion so that you don’t absorb glucose from your food as quick.
The Ketogenic Diet for Type-1 Diabetes
The ketogenic diet can be a powerful management tool for type-1 diabetes. Based on the resources available to date, very low carbohydrate diets have shown to offer profound glycemic control, all while requiring less insulin and producing fewer side effects to standard approaches. Lower insulin requirements reduce risk for error as mentioned previously – a point that should not be overlooked given the severity of complications that can occur. Perhaps the most compelling evidence is the data published in 2018 from the online community, “Type-1 Grit” – a group of type-1 diabetics following very low carbohydrate diets [3]. This is a group of individuals following the guidance of the book: Dr. Bernstein’s Diabetes Solution, by Richard K. Bernstein, MD, and while not explicitly ketogenic, the carbohydrate consumption averaged ~36g/day. The study involved 316 participants who met the criteria of inclusion. The results demonstrated impressive glycemic control in that the diet produced an average HbA1c* within the normal to near-normal range, values only ~1.3% of type-1 diabetics achieve [4]. Additionally, low rates of hypoglycemic events and/or other adverse side effects were reported. The authors credit the outcomes to the reduction in postprandial elevations in blood glucose and the lower insulin doses required with a very low carbohydrate diet.
Very-low carbohydrate diets do not replace insulin, rather they offer a way to make management easier and safer for most. The goal with this style of eating is glycemic control, and ketosis is not always achieved. However, the common concern with carbohydrate restriction in type-1 diabetics is the risk of ketoacidosis. Ketoacidosis is a pathological state that can occur in the complete absence of insulin, but the low to moderate amount of insulin still required on very-low carbohydrate diets is sufficient enough to prevent ketoacidosis.
More rigorous trials are absolutely needed to confirm just how effective very low carbohydrate diets can be for type-1 diabetics and any potential long-term side effects, but with the current data, it certainly appears to be a safe and effective tool for glycemic control. Above all, is the potential to reduce insulin, better predict appropriate insulin dosing, and reduce the risk of blood glucose fluctuations, a major feat to a type-1 diabetic.
*HbA1c is the marker used to determine average blood glucose levels over a 2-3-month period, also used for diabetes diagnosis.
For a deep dive on type-1 diabetes and very-low carbohydrate diets, we recommend visiting www.andrewkoutnik.com.
The Ketogenic Diet for Type-2 Diabetes
The evidence to support a ketogenic diet for type-2 diabetes deserves much more attention than what it has been given. The diet has proven that reversal is possible [5], and it is saddening to think that most patients are told they will have the disease for life. Over the past two decades, several studies of carbohydrate restriction have reported profound benefits for type-2 diabetes. The findings are consistent in that the lower the carbohydrate content of the diet, the better the outcomes [6], reflecting the strong association between dietary carbohydrates, insulin resistance, and type-2 diabetes. The most recent analysis of low carbohydrate diets for type-2 diabetes highlights multiple studies ranging from 2-week interventions to 2-years, demonstrating reductions in HbA1c values, improvements in glycemic control, and weight loss [5]. Most notably is the reduction in diabetes medications, to the point in which many patients have completely eliminated them.
Despite benefits being reported independent of weight loss, obesity is tightly linked to type-2 diabetes, and the weight loss effect of a ketogenic diet can therefore be a major benefit for these patients. In fact, obesity is one of the biggest drivers of insulin resistance and type-2 diabetes. Therefore, the ketogenic diet not only targets blood glucose control but also weight management, simultaneously.
Conclusion
Very-low carbohydrate ketogenic diets are a tool to better manage glucose in both type-1 and type-2 diabetics as outlined here. The diet essentially reduces the glycemic load of the diet via carbohydrate restriction, reducing postprandial glucose excursions, medication requirements, and therefore preventing large fluctuations in blood glucose. The current standard approach to diabetes management appears to be failing us given the low rates of glycemic control and disconnect from the dietary impact on blood glucose. Although maybe not for everyone, the ketogenic diet and carbohydrate restriction should not be discounted as unrealistic or too restrictive, as the effects of the diet not only offer quantitative improvements, but can truly enhance quality of life. Both the short- and long-term consequences of poorly managed diabetes require more attention, so that strategies such as ketogenic diets can gain greater attention by the medical communities. In addition to all of this, reducing or eliminating diabetes medications can be a huge cost saving to both individuals and our health care systems.
We strongly believe this dietary strategy should not be withheld from patients upon diagnosis, as it is within their best interest to have access to this information given the benefits realized to date. Trials are ongoing and many clinics are utilizing low carbohydrate diets with success in patients. This keeps us hopeful for future improvements to the current recommended guidelines to support ketogenic diets for both type-1 and type-2 diabetes.
To wrap it up, we will leave you with a quote from Dr. Eric Westman, MD, who continues to demonstrate the use of ketogenic diets in diabetic patients:
“At the end of our clinic day, we go home thinking that the clinical improvements are so large and obvious, why don’t other doctors understand? Carbohydrate restriction is easily grasped by patients. Because carbohydrates in the diet raise the blood glucose, and as diabetes is defined by high blood glucose, it makes sense to lower the carbohydrate in the diet. By reducing the carbohydrate in the diet, we have been able to taper patients off as much as 150 units of insulin per day in 8 days, with marked improvement in glycemic control—even normalization of glycemic parameters.”
—Eric Westman, MD, MHS [7]
If you are considering carbohydrate restriction to improve your diabetes, talk with your health care professional first. Close management of glucose and ketones to achieve a normal Hba1c, normal lipid levels, and lowering of medication(s) should be your goals. Share the resources below with your provider to educate them about the latest research on ketogenic diet therapies for diabetes.
Resources:
- Sansum WD, et al. 1928. The use of high carbohydrate diets in the treatment of diabetes mellitus. JAMA, 86:178-181.
- Newburgh LH, et al. 1920. The use of high fat diet in the treatment of diabetes mellitus. Arch Intern Med (Chic), 26(6):647-662.
- Lennerz BS, et al. 2018. Management of Type 1 Diabetes with a very low-carbohydrate diet. Pediatrics, 141(6).
- Exchange, T. D. T1D Discovery Tool. https://t1dexchange.org/
- Hallberg SJ, et al. 2019 Reversing type 2 diabetes: a narrative review of the evidence. Nutrients, 11(4):766.
- Sorgaard O, et al. 2017. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Research and Care, 5:e000354.
- Westman EC and Vernon MC. 2008. Has carbohydrate-restriction been forgotten as a treatment for diabetes mellitus? A perspective on the ACCORD study design. Nutr Metab (Lond), 5:10.